Regional Grants
The GROW (Growing Rural Opportunities for Well-being) initiative brings the federal RHTP program to the state level. Indiana understands that rural communities know their own needs best and are well-positioned to create effective local solutions. The state has a strong track record of helping communities use data to identify their biggest opportunities and leverage local resources and partnerships to address them.
Activity
In Progress
- RHT-TAN continuing to meet with Regional Coalitions to support the RFF Applications submitted July 1 now under review.
Completed
- Eight Regional Grant Coordinators hired
- Bi-weekly Regional Committee meetings (ONGOING)
- Regional submissions of Letters of Intent
- Establish GROW Regional Committees
- Release RFF on 3/2/26
- Develop RFF Application
- Formalize Technical Assistance Partnership (RHT-TAN)
|
Template |
Document |
Purpose |
|
Provide all details regarding the GROW Regional Grants, including background, funding opportunity overview, application requirements and expectations. |
||
|
A |
Identify all Regional Coalition members who are expected to be Primary Subrecipients and provide attestation that all eligible counties within the region are represented. Due by May 22, 2026. |
|
|
B |
Demonstrate how proposed initiatives are responsive to documented community needs and how they will further Indiana’s Rural Health Transformation Program KPOs. |
|
|
C |
Provide a roadmap connecting a Regional Coalition's identified needs and proposed Initiatives to region-specific outcomes. |
|
|
D |
Detail implementation timeline, Primary Subrecipient roles, and milestones. |
|
|
E.1 |
Primary Subrecipient Budget Workbook to capture each Subrecipient's proposed costs. |
|
|
E.2 |
Regional Grants Budget Workbook to capture all proposed costs for a region. |
|
|
F |
Final step in the application, providing an opportunity for the Regional Coalitions to cohesively tell their story. |
|
Appendix |
Document |
Purpose |
|
1 |
Provides an overview of CMS’ expectations for states for overall awareness on the Rural Health Transformation Program. |
|
|
2 |
Provides a few examples of Initiatives and their associated activities to guide Regional Coalitions in structuring their proposed projects. |
|
|
3 |
Provides a list of pre-approved outcome measures and metrics for primary use in the Logic Model Completion. |
|
|
4 |
Provides an overview of the Allowable and Unallowable Uses of Funds per CMS as a reference tool as the Regional Coalitions put their applications together. |
|
|
5 |
Outlines the RHTP Indiana and GROW Regional Grants governance frameworks, roles and oversight responsibilities. |
|
|
6 |
Use this checklist as a guide to ensure all application elements are completed. |
|
| Regional Grant Budget Period Planning Worksheet | Provides timelines of future Budget Periods and key themes for program planning in Budget Period 1 and later Periods. Includes template pages outlining Associated Activities, specific investments, and key stakeholders in each program phase. |
Program Overview
RHTP GROW Regional Presentation
Indiana will offer competitive regional grants focused on improving rural health. These grants will support:
- Innovative health solutions
- Collaboration to reduce costs across organizations
- New access points for preventive care
- Chronic disease prevention and management
- Workforce training and readiness
- Technological advancements in healthcare
To qualify for funding, participating organizations must fully engage with the expectations outlined in Indiana RHT’s broader initiatives.
Regional Committees
The Regional Committee is an advisory team within each region appointed by the State Executive Oversight group.
They will represent key rural health stakeholders, utilizing subject matter expertise to assess potential beneficiaries of the GROW Regional Grants to ensure accountability and an equitable distribution of funds.
The Regional Committee must meet at least quarterly to provide strategic guidance, foster regional collaboration, drive accountability, and review regional progress and impact. The Regional Committees will review regional applications before they are submitted to the state.
Each Committee must include:
- 1 Member of the Indiana General Assembly
- 1 Provider Representative
- 1 Non-Provider Medical Workers Representative
- 1 Patient Representative
- 1 Pharmacy Representative
- 2 Regional Business Community Representatives
- 2 Community-based Organizations Representatives
- 1 Local Health Department Representative
- 1 Medicaid Managed Care Representative
- 1 Rural Hospital
- 1 Specialty Obstetric Care Representative
Region 1 | Name | Hospital/Organization |
| General Assembly | Rep. Mike Aylesworth | District 11 |
| Physician | Dan Nafziger | Goshen Health |
| Non-Physician | Jen Shafer | Pulaski County Recovery Café & Circuit Court |
| Patient | TBD | TBD |
| Pharmacist in the Community | Bryan Mumaugh | Franciscan Hospital |
| Business | Gary Neidig | One Marshall County |
| Business | TBD | TBD |
| Community-based Organization | Jennifer Malone | CoAction |
| Community-based Organization | Katie Surma | Jasper-Newton Community Support Network |
| Local Health Department Staff | Melanie Sizemore | Elkhart County Health Officer |
| Medicaid Managed Care Representative | Darryl Lockett | Anthem |
| Rural Hospital Staff | Steve Jarosinski | Pulaski Memorial |
| Specialty Obstetric Care Representative | April Rantz | Woodlawn Hospital |
Region 2 | Name | Hospital/Organization |
| General Assembly | Rep. Craig Snow | District 22 |
| General Assembly | Sen. Justin Busch | District 16 |
| Physician | Sara Brown | Parkview Health |
| Non-Physician | Jared Beasley | Community Health Clinic |
| Patient | Mark Demchak | Miami County YMCA |
| Pharmacist in the Community | Tara Jellison | Parkview Health |
| Business | Natalie DeWitt | Taylor Rental |
| Business | TBD | TBD |
| Community-based Organization | Ann Lundy | Indiana Health Centers |
| Community-based Organization | Steve Hoffman | Brightpoint |
| Local Health Department Staff | Matt Pflieger | Huntington County Health Department |
| Medicaid Managed Care Representative | Dustin Ziegler | Anthem, Indiana PathWays |
| Rural Hospital Staff | Angie Logan | Cameron Health |
| Specialty Obstetric Care Representative | Todd Rumsey | Cameron Health |
Region 3 | Name | Hospital/Organization |
| General Assembly | Rep. Matt Commons | District 13 |
| Physician | Eric Frantz | St. Vincent Williamsport |
| Non-Physician | Melissa Hodson-Ostler | Clinton County Health Department |
| Patient | Lorra Archibald | Healthy Communities of Clinton Co |
| Pharmacist in the Community | Katelyn Riddell | Butler University & Cowan Drugs |
| Business | Macy Simmons | Integrative Wellness |
| Business | Gina Woodward | MICI AHEC |
| Community-based Organization | Holly Wood | Purdue University |
| Community-based Organization | Chad Springer | North Central Nursing Clinics (Purdue University) |
| Local Health Department Staff | Christine Rodziewicz | White County Health Department |
| Medicaid Managed Care Representative | Christina Hage | Managed Health Services (MHS) |
| Rural Hospital Staff | Carlos Vasquez | Franciscan Health Rensselaer, Franciscan Health Crawfordsville |
| Specialty Obstetric Care Representative | Faihza Hill | IU Health Primary Care |
Region 4 | Name | Hospital/Organization |
| General Assembly | Sen. Jeff Raatz | District 27 |
| Physician | Jennifer Bales | Reid Health |
| Non-Physician | Shelley Dunham | Ascension St. Vincent Anderson |
| Patient | Karen Hinshaw | Indiana University School of Medicine |
| Pharmacist in the Community | Cheri Knapke | IU Health |
| Business | Clark Simpson | YMCA of Madison County |
| Business | Linda S. Fitzgerald | Healthy Fayette County |
| Community-based Organization | Amanda Mullins | Centerstone - Community Mental Health |
| Community-based Organization | Billie Wolfe | ECI-AHEC |
| Local Health Department Staff | Shae Bex | Henry County Health Department |
| Medicaid Managed Care Representative | Jessica Parks | Managed Health Services (MHS) |
| Rural Hospital Staff | Stephanie Hilton-Siebert | Marion Health |
| Specialty Obstetric Care Representative | Amber Liles | Ascension St. Vincent Anderson |
Region 5 | Name | Hospital/Organization |
| General Assembly | Rep. Beau Baird | District 14 |
| Physician | Michael Gamble | Sullivan Health Department |
| Non-Physician | Jennifer Knight | Greene County Ambulance Service |
| Patient | Paul Sinders | Clay County Government |
| Pharmacist in the Community | Ryan Chavis | Union Hospital Clinton |
| Business | Amy Mace | Cummins Behavioral Health |
| Business | Art Fuller | Hamilton Center, Inc. |
| Community-based Organization | Terry (TJ) Warren | Valley Professionals Community Health Center |
| Community-based Organization | Amanda Perry | Richard Lugar Center for Rural Health |
| Local Health Department Staff | Shari Lewis | Greene County Health Department |
| Medicaid Managed Care Representative | Dana Moell | Managed Health Services (MHS) |
| Rural Hospital Staff | Michelle Franklin | Sullivan County Community Hospital |
| Specialty Obstetric Care Representative | Summer Appling | IU Health |
Region 6 | Name | Hospital/Organization |
| General Assembly | Rep. Alex Zimmerman | District 67 |
| General Assembly | Rep. Garrett Bascom | District 68 |
| Physician | Holly Robinson | Infants in Bloom |
| Non-Physician | Rex McKinney | Decatur County Memorial Hospital |
| Patient | Kathy Ertel | Jennings County Economic Development |
| Pharmacist in the Community | Anna Lattos | St. Elizabeth |
| Business | Will Gott | Wood-Mizer |
| Business | Sonja White | Batesville Tool and Die |
| Community-based Organization | Elizabeth Boyd | New Hope |
| Community-based Organization | Tara Britton | Southeastern Indiana YMCA |
| Local Health Department Staff | Sean Durbin | Decatur County Health Department |
| Medicaid Managed Care Representative | Brittany Burtraw | Care Source |
| Rural Hospital Staff | Liz Leising | Margaret Mary Health |
| Specialty Obstetric Care Representative | TBD | TBD |
Region 7 | Name | Hospital/Organization |
| General Assembly | Sen. Eric Koch | District 44 |
| Physician | Kalen Carty-Kemker | Ascension |
| Non-Physician | Amy Meek | IU Health Community |
| Patient | Dan Robinson | Jackson County Chamber |
| Pharmacist in the Community | Kellie Knight | IU Health in Southern Indiana |
| Business | Dan Peterson | Cook Group Incorporated |
| Business | Andy Zirkle | Indiana Health Centers, Inc. |
| Community-based Organization | Beth Keeney | LifeSpring Health |
| Community-based Organization | Andrew Settle | YMCA of Harrison County |
| Local Health Department Staff | Lonnie Stroud | Orange County Health Department |
| Medicaid Managed Care Representative | Mark Vonderheit | Managed Health Services (MHS) |
| Rural Hospital Staff | Lisa Lieber | Harrison County Hospital |
| Specialty Obstetric Care Representative | Eric Fish | Schneck Hospital |
Region 8 | Name | Hospital/Organization |
| General Assembly | Rep. Tim O'Brien | District 78 |
| Physician | Nick Dahl | Daviess County Primary Care Physician |
| Non-Physician | Paul Micheletti | Posey County EMS |
| Patient | Jessica Kincaid | Spencer County Health Coalition |
| Pharmacist in the Community | Carrie Morton | Deaconess Health Systems |
| Business | TBD | TBD |
| Business | TBD | TBD |
| Community-based Organization | Lloyd Winnecke | Evansville Regional Economic Partnership |
| Community-based Organization | Nikki Lasher | Tri-Cap |
| Local Health Department Staff | Kellie Streeter | Daviess County Health Department |
| Medicaid Managed Care Representative | Sarah Jo Poland | UnitedHealthcare |
| Rural Hospital Staff | Adam Thacker | Good Samaritan |
| Specialty Obstetric Care Representative | Sarah Morrison | Good Samaritan |
Regional Application Development and Timeline
The Indiana Health and Family Services (HFS) is creating the GROW Regional Grant Application to align with federal RHTP guidelines. This application will provide clear, step-by-step guidance for applicants on how to identify and address the unique health needs of rural communities.
The goal is to advance rural health across Indiana in line with CMS’ strategic priorities —focusing on data-driven solutions, strong partnerships, innovation, and long-term sustainability.
To ensure a smooth and transparent process, HFS will partner with an experienced grant-making vendor to assist with:
- Developing the application
- Designing evaluation criteria (with final award decisions made by the state)
- Creating grant agreements
- Setting clear expectations for outcomes and financial reporting
| Indiana Regional Grant Application Timeline | |
|---|---|
| Date | Milestone |
| March 2026 | Request for Applications released to public |
| March -- July 2026 | Technical assistance available for coalition formation and application development |
| May 22, 2026 | Letters of Intent due to State |
| July 1, 2026 | Applications due to State |
| July -- September 2026 | Application review, scoring, and award determinations |
| Sept. 1, 2026 | Grant agreement period begins, and funding distributed to individual entities |
Regional Grant funding timeline is different than overall state funding timeline.
Pre-Application Expectations
The Regional Coalitions are encouraged to begin identifying partners, convening discussions about shared regional rural priorities, conducting joint needs assessments, and exploring data sharing agreements. Regional Coalitions demonstrating preliminary planning and established governance will be better positioned to rapidly deploy funding upon contract award.
Transforming Rural Health Through Regional Collaboration
Indiana is planning to invest $600 million over five years based on CMS RHTP award each year, to transform rural healthcare through a Regional Coalition Grant Model — a strategy designed to achieve what state-led efforts cannot. This model brings together hospitals, federally qualified health centers (FQHCs), mental health providers, community-based organizations, local health departments, schools, the business community, and other key partners to strengthen healthcare delivery across rural Indiana.
Unified Regional Applications
Each region will submit a single, unified application that demonstrates a shared plan for improving health outcomes. Applications must use community needs assessments and local health data from the Indiana Department of Health (IDOH) to identify service gaps, reduce duplication, find opportunities for shared cost savings, and propose innovative ways to deliver care.
By requiring one coordinated application per region, the program ensures that these partnerships extend beyond the grant period, forming the foundation for long-term regional health planning. Funding will be distributed directly to the organizations carrying out the initiatives. This approach recognizes that rural providers understand their communities best and that collaboration leads to lower costs, fewer service gaps, and better patient outcomes.
Regional Grant Oversight and Governance
The state will maintain strong oversight while giving rural communities the flexibility they need to innovate. The Indiana Health and Family Services (HFS) will ensure that all sub-grantees comply with Notice of Funding Opportunity (NOFO) and Centers for Medicare & Medicaid Services (CMS) guidelines, state grant rules, and reporting requirements. Public dashboards and key performance tracking will make data transparent and hold each region accountable for results.
Oversight will be led by two main committees. The Executive Oversight Committee, made up of leaders from Health and Family Services and the Governor’s Office, will have final authority over application approvals, funding decisions, and performance monitoring. It will oversee the grant throughout its duration and adjust funding annually based on compliance and outcomes. The State Steering Committee, jointly staffed by the Family and Social Services Agency (FSSA) and IDOH, oversees all activities, progress, and risks across the full Program.
The RHTP Advisory Committee serves in a strictly advisory capacity, leveraging unique knowledge and skills to offer expertise; offer recommendations and insight to inform the State Steering Committee; facilitate connections both statewide and for Regional Grants, including community partners, and other relevant entities; and propose support/solutions for specific initiatives when needed to navigate complexities of the initiatives.
| Name | Role | Type of Organization | Organization |
|---|---|---|---|
| Anne Hazlett, JD, LLM | Senior Director of Governmental Relations and Public Affairs | Public University | Purdue University |
| Cara Veale, DHS, FACHE | Chief Executive Officer | Statewide Healthcare Association | Indiana Rural Health Association |
| Andy VanZee, MHA, MIS, FACHE | Vice President, Regulatory & Hospital Operations | Statewide Healthcare Association | Indiana Hospital Association |
| Ben Harvey | Chief Executive Officer | Statewide Healthcare Association | Indiana Primary Health Care Association |
| Cameual Wright, MD, MBA | President | Medicaid Managed Care Entity | CareSource Indiana Market |
| Charlotte MacBeth | Vice President, Provider Network | Commercial Insurer | UnitedHealth Group |
| Steve Howell, MS, LMHC, LCAC | Chief Executive Officer | Certified Community Behavioral Health Center | Northeastern Center |
| Rex McKinney, MBA, FACHE | President/CEO | Rural Hospital | Decatur County Memorial Hospital |
| Eric Fish, MD, MBA | President/CEO | Rural Hospital | Schneck Medical Center |
| Kamal Girgis, MD | Internist and Hospitalist | Rural Practice | IU Health Bedford |
Regional Grant FAQs
This initiative duplicates the federal RHTP at the state level. It aims to reduce healthcare gaps and costs, foster regional partnerships, and advance rural health outcomes in alignment with CMS goals. It launches Sept. 1, 2026, with $120M awarded annually across eight regional coalitions.
How can my organization sign up for funding?
Organizations cannot apply alone; they must participate as part of a regional coalition. Each of the eight regions will submit one unified application that includes all proposed projects and subrecipients. Organizations should connect with their regional partners to be included in their region’s application.
Where do regions submit their letter of intent and other application materials?
Your Technical Assistance Provider will provide guidance on how to submit these materials.
If a region is unable to submit the application by the deadline, does it have any recourse?
The default expectation is that applications are due July 1, 2026, and late submissions will not be accepted. If a region faces extraordinary circumstances, it must notify HFS as early as possible during the technical assistance period (March–July 2026). Any accommodation would be rare, case-by-case, and at the discretion of the State Executive Oversight Committee.
What data should regions examine to prepare for their applications?
At a minimum, regions should review:
- Local health outcome data (chronic disease, maternal and infant health, behavioral health, preventable ED visits)
- Access and capacity data (workforce, facility availability, travel times, service gaps)
- Non-medical needs data (transportation, food access, housing, broadband)
- Existing program and infrastructure maps (what already exists, where duplication or gaps occur)
IDOH will provide regional data snapshots which regions are expected to use to anchor their needs assessments.
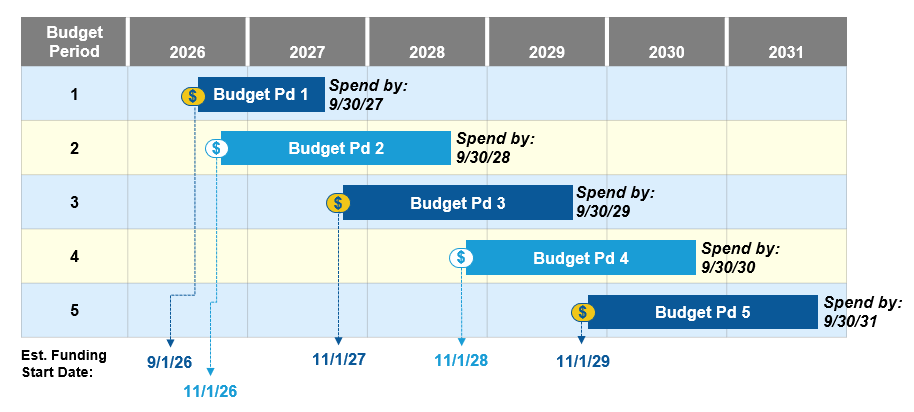
Since money will be coming to regions on Sept. 1, 2026, how long do the regions have to spend their money?
The Regional Grants are designed as a five-year funding period (FY27–FY31), with funding distributed annually starting Sept. 1, 2026. Regions will receive annual allocations, and funds must be spent within each grant year in alignment with approved budgets, with limited flexibility for carryover as permitted by state and federal rules. The regional grant funding amount awarded to each region each year may be recalibrated based on the overall recalibration of Indiana awarded funds, which occurs each November, effective that federal fiscal year.
Will regions receive funding for administrative costs?
Yes. Reasonable administrative and program management costs at both the regional and organizational level are allowable, as long as they:
- Are clearly described in the budget.
- Are necessary for program implementation, oversight, and reporting.
- Stay within any indirect cost limits set by CMS and the state.
Is grant administration/committee leader salary an allowable expense within this grant?
Committee leaders will not be permitted to draw a salary from RHTP grant budgets. However, some direct administrative costs may be allowable for funded organizations receiving RHTP funds to manage and administer the grant.
When will the application for regional grants be released?
The application is available now and can be found at the top of this page.
What is the criteria for applications?
According to the RFF, applications must include all five required templates, be complete, and be submitted by the deadline.
The application must include the following five required components:
- Needs Assessment (Template B)
- Logic Models (Template C)
- Implementation Workplan (Template D)
- Budget Workbooks (Templates E.1 & E.2)
- Initiative Narrative Response (Template F)
Additional application criteria include:
- Submission of a Letter of Intent (Template A) by May 22, 2026.
- Use of the Needs Assessment to justify selected initiatives.
- Alignment with at least one of the five Funding Categories (tech innovation, sustainable access, innovative care, workforce development, and Make Rural Indiana Healthy Again).
- Addressing required health outcomes unless strongly justified otherwise (prenatal/postnatal care, chronic disease prevention and management, and access-related needs such as transportation or food access).
How are applications scored?
Applications are scored using two major components: base funding allocation and application evaluation criteria. Only the second component is based on the quality of the application.
1. Base funding allocation (80% of total award)
This portion is not scored by the application, but by state-calculated data indicators:
- Population size (80%)
- Access to healthcare (10%), based on:
- Health professional shortage area designation (60%)
- Medically underserved area/population designation (40%)
- Health indicators (10%), including Medicaid enrollment, infant mortality, diabetes, obesity and life expectancy
2. Application evaluation criteria (20% of total award)
This score directly depends on the strength of the submitted application and is assessed based on the five categories listed in Figure 7 of the RFF:
- Strategy – How transformative and impactful the proposed investments are.
- Workplan & Collaborative Structure – Clarity, feasibility, partner coordination and oversight structure.
- Outcomes – Specificity, measurability and grounding in credible evidence.
- Projected Impact – Expected benefit to rural residents and scale of impact.
- Sustainability Beyond Funding – Strength and plausibility of long-term sustainment plans.
Each category includes descriptors for Weak, Acceptable, Strong and Exceptional responses. Stronger responses lead to a larger share of the $24 million available through competitive scoring. The State will convene an application review team that will score applications and determine funding amounts according to the guidance included in the application.
Who will issue the grant awards and where will this be posted?
Grant awards will be issued by the Indiana Department of Health and posted to the Indiana RHTP website.
How much funding is each region receiving?
The funding amounts are still to be determined.
When are the applications due?
Applications will be due July 1.
Will there be informational sessions by region? In person/webinars?
Yes. Please reach out to the GROW T/A providers for information about upcoming virtual sessions.
When will grant awards/projects be announced?
Grant awards will be announced no later than Sept. 1.
How do I know what other projects are being submitted or considered? How do I ensure I am included?
Please work with your Regional Coalition to participate in the application development project. Watch the Indiana RHTP website for updated information on the TA providers that will help facilitate this process.
If my project is submitted to the regional coalition and included in application, how do I get my money?
If your organization’s project is submitted as part of the regional application and approved, you will be awarded funding from the Indiana Department of Health through a subgrant contractual agreement.
If I submitted a project and I have multiple partners included in my project, will I receive all the money?
Primary subrecipients will be prohibited from awarding funds granted by the State to other subrecipients via sub-awards/sub-grants. Primary subrecipients may still award funds to contractors.
How do we determine what promotional items are allowable?
Allowed Items: Materials that support access, navigation, safety or health outcomes. Examples include brochures, rack cards, navigation guides, magnets with clinic hours, posters, instruction cards, safe sleep cards, medication logs, telehealth instructions, appointment prep sheets, and items required for participation (e.g., BP cuffs as part of approved RPM activities).
What promotional items are not allowable?
Not Allowed: Items that do not support program outcomes, even if branded. Examples include stress balls, pens, clothing, water bottles, tote bags, stickers, toys, decorative items, food giveaways, buttons, and any merchandise meant to increase visibility rather than support access.
How will applications be assessed, and who conducts the review?
Regional grant applications will be reviewed through a competitive scoring process led by the GROW State Steering Committee, and their designees. Proposals will be scored on factors such as:
- Strength and breadth of the regional coalition
- Data-driven needs assessment
- Alignment with required categories and KPOs
- Evidence of non-duplication and filling gaps
- Quality of sustainability and governance plans
- Commitment to participation in statewide RHTP initiatives (further clarification on regional grant participation is outlined in the RFF)
All eight regions are expected to receive funding, but award size will vary by population served and quality of application.
How will the state ensure the use of AI in reviewing regional applications is fair? Will AI be used?
The core scoring and funding decisions will be made by human reviewers. The state may use technology tools (including limited AI or analytics) to assist with tasks such as consistency checks or data aggregation, but no application will be approved or denied solely by an AI system. Any use of AI will be transparent, standardized, and overseen by human reviewers to protect fairness.
Just to clarify, the regions don't self-select the regional committees, but the state executive oversight selects the individuals who will make up the regional committees? Who is going to certify the submission groups?
HFS will work with state associations to identify individuals who will lead the Regional Coalitions and the Regional Committee members. The State Executive Oversight Committee will approve the composition of each Regional Committee based on required roles (e.g., rural hospitals, provider, non-provider medical worker, CBOs, patient, LHD, Medicaid MCO, business, pharmacy, legislator). The same executive body (or its designee) will certify each Regional Coalition as eligible to submit a unified regional application.
How are committees ensuring the right people are included in decision-making? What does it mean for regional community members who volunteer?
Each Regional Committee must include specific stakeholder types (e.g., rural hospitals, CBOs, patient representative, LHD, Medicaid MCO, business sector). Community members or groups who volunteer will be considered during committee formation and can:
- Serve in required roles (e.g., CBO, patient representative)
- Participate in advisory councils, workgroups, or project design processes
Final membership is approved by the State Executive Oversight Committee to ensure balanced representation and avoid dominance by any single entity.
How does the overall governance structure work together?
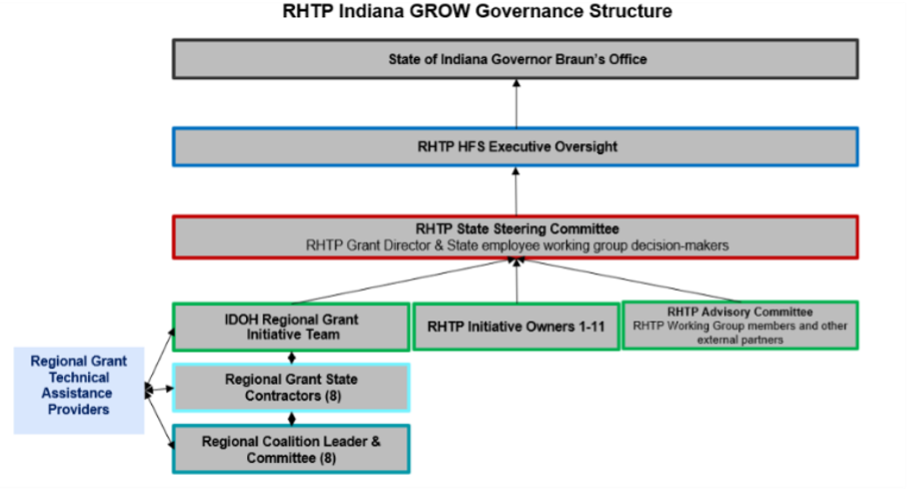
- Governor / State Executive Oversight Committee: Final authority over awards, compliance, and course correction.
- RHTP State Steering Committee: Reviews progress, advises on strategy, and lifts cross-regional issues.
- IDOH Regional Grant Initiative Team: ongoing oversight of regions throughout grant period; state management of contracts, grant agreements, leads application review and scoring and makes funding recommendations with final approval by the State Executive Oversight Committee.
- Regional Grant State Contractors: Serve as the coordinator of all activities associated with the regional activities, direct communication with IDOH Regional Grant Initiative Team for clarifications and escalations as needed.
- Regional Coalition Leader: Design, prioritize, and oversee projects within their region; monitor budgets and outcomes; ensure alignment with state requirements.
- Regional Committees: ongoing strategic guidance to regional coalitions – must approve application before submission to state.
- Regional Grant Technical Assistance Provider (state-contracted): will provide application assistance, performance monitoring, and cross-regional learning support.
Governance is layered so decisions are locally informed but state-accountable.
Once the committees are formed and their proposal is submitted this summer, will they direct the process for surrounding institutions/health systems/providers to potentially partner achieving their outcomes? Or as a health system, do we need to contact the state/committee to participate?
Once Regional Committees are set and proposals are submitted, they will identify partners and aligning regional activities with the outcomes outlined in their proposals. Participation is not limited to organizations already at the table. Health systems and other providers that wish to be involved should proactively reach out to the Regional Committee or to the regional grant technical assistance providers.
Can you share more information about data collection, tracking success and measuring results?
Data collection and performance measurement will follow a standardized, statewide framework to ensure consistency across all regions. Each Regional Coalition will track progress toward the outcomes identified in its proposal using a mix of health indicators, system‑capacity measures, and implementation metrics. The state will provide templates, technical assistance, and shared reporting tools to support this work, and regions will submit regular updates that highlight progress, challenges, and opportunities for improvement. The goal is to create a clear, practical approach to monitoring results that strengthens accountability while supporting continuous learning and adaptation.
Does the coalition stay in place for the five year period?
Yes.
How is rurality being assessed/defined?
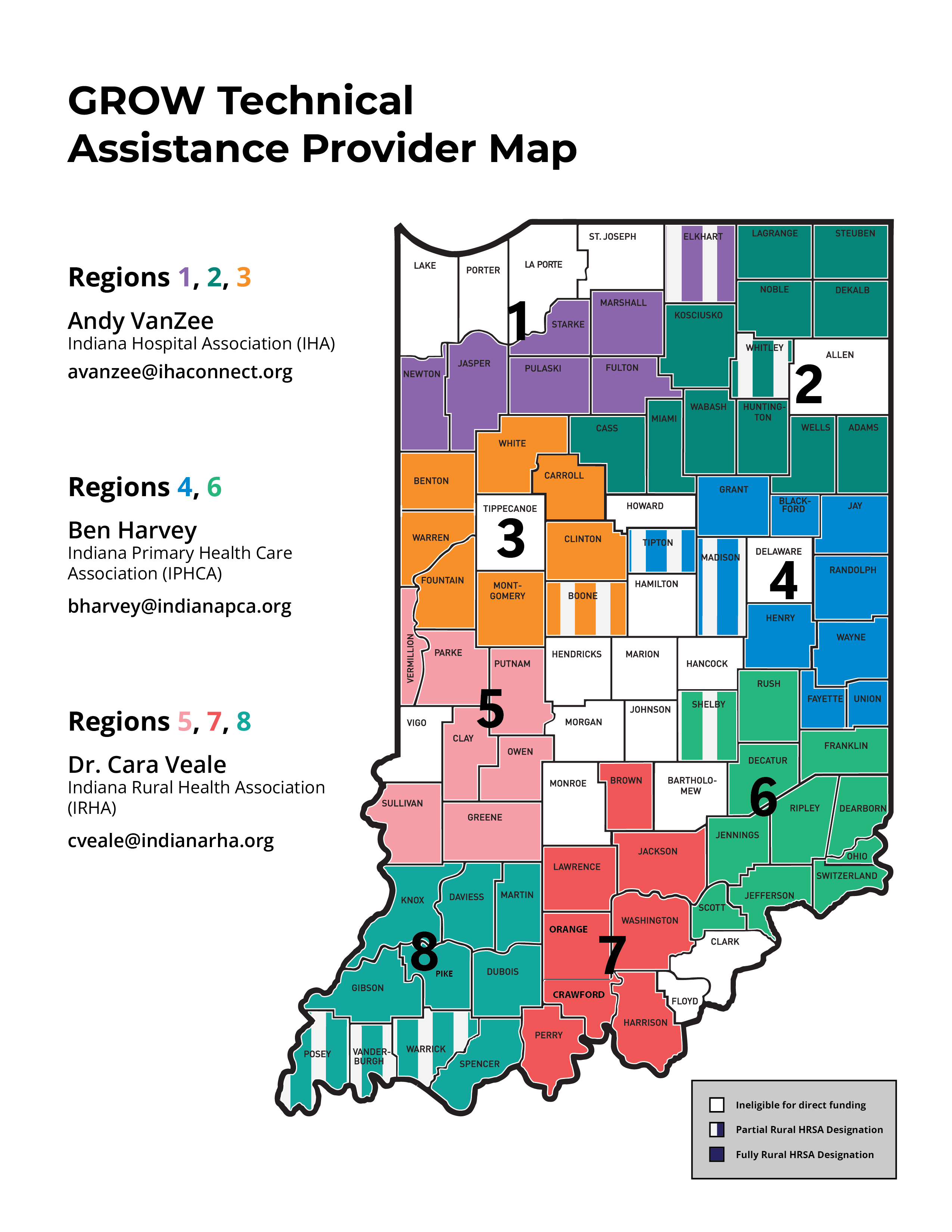
Counties with HRSA Rural Designation are considered fully rural and organizations within those counties may be direct recipients of the RHTP funds as part of the regional application. Organizations in these counties should be prioritized in regional coalitions and subsequent applications. These 64 counties are noted in the regional map as solid-colored counties.
There will be nine additional counties which may also be considered direct recipients eligible for RHTP funds as noted with stripes in the regional map. The stripes indicate a county has either a HRSA rural designation with a distinction that only some parts of the county are eligible for rural health grants; or a non HRSA rural designated county, but has a HRSA designated critical access hospital. It is important to note that organizations in metropolitan areas within the striped counties will only be funded with justification as to how they are serving rural residents. Regional applications should provide this detailed explanation within the work plan narrative. Partially rural counties are identified as counties eligible for funding directly from the RHTP grant.
Will the regions mirror existing public health preparedness districts? If not, have those lines been drawn yet?
The Rural Health Regional Map is based on the HRSA designation of counties in Indiana eligible for rural health grant funding. From there, the eight regions align with natural care/referral patterns and trauma/preparedness regions.
How can we ensure rural hospitals are represented on the Regional Committees?
Each Regional Committee is required to include at least one healthcare provider representative, and the program strongly expects that in rural-focused regions, this role will be filled by a rural hospital or rural health provider organization. Regions will be encouraged to involve multiple rural hospitals as subrecipients and advisory partners, even beyond the minimum committee seat.
How can we ensure community mental health centers/CCBHCs are represented?
Community mental health centers and CCBHCs are explicitly identified as key stakeholders throughout GROW and can serve as:
- Provider representatives on the Regional Committee
- Subrecipients for behavioral health projects
- Leads or co-leads on behavioral health and workforce initiatives
The State will strongly encourage behavioral health representation in both the committee membership and project portfolio.
What should the involvement for non-rural counties be?
Non‑rural counties are not the target of RHTP funding, but their involvement should be part of improving outcomes in rural counties. Some examples include serving as a partner when service area supports rural outcomes, contribute training and workforce development, specialty care access or participate in other initiatives that span more than one county, such as behavioral health integration or maternal health readiness.
Will there be a forum where the districts can learn from each other in the first few months during the application development process?
Not at this time, but this request can be made to the GROW Regional Grants technical assistance providers. Information about these providers will be shared soon.
When there is not agreement on the regional committee plan, who steps in to support conflict resolution?
The GROW Regional Grant technical assistance providers will assist in convening and facilitating coalition formation and application development. Ultimately it will be the responsibility of the Regional Coalition and Committee to find consensus and submit a proposal that benefits rural residents within each region.
If not selected to be part of a regional committee, what will be the process for active participation in the application process and/or to provide input. Will someone from the region be reaching out to organizations?
All regional stakeholders should be part of the application process, even if they are not part of the Regional Committee. The GROW Regional Grant technical assistance providers will help facilitate this collaboration.
Will the technical assistance team convene potential partners in our region soon, to begin the planning process? The timeline is aggressive unless relationships already exist across the region.
Yes. Please reach out to the T/A provider for your region to be included in the planning sessions.
When will regional committee members be announced?
The Regional Committee members are listed at the top of this page.
What is the role of the regional committees?
Regional Committees are the governing and advisory group for each region, similar to a board of directors. Comprised of 13 appointed members, their role is to ensure diverse representation for the Regional Coalition, provide guidance, and receive regular updates on progress. They do not develop or implement the regional plan but provide counsel, help maintain alignment with regional priorities, and support transparent communication between the Coalition and the community.
Who are the T/A providers, what is their role, who are the contacts?
The Indiana Rural Health Association (IRHA), Indiana Hospital Association (IHA) and Indiana Primary Health Care Association (IPHCA) are providing technical assistance to regions as the coalitions determine their needs, design initiatives and prepare their applications. See the map above to see who your T/A provider for your region is, or see below:
- Regions 1, 2, 3: Andy VanZee, IHA, avanzee@ihaconnect.org
- Regions 4, 6: Ben Harvey, IPHCA, bharvey@indianapca.org
- Regions 5, 7, 8: Dr. Cara Veale, IRHA, cveale@indianarha.org
Whom do I reach out to with questions in my region?
Contact your T/A provider for your region listed above.
What types of costs are allowed and what are not allowed? Clearly identify and explain the parameters for Indiana Regional Coalitions spending GROW money.
In general, eligible costs must:
- Directly support access, technology innovation, workforce development, MRAHA, or innovative care
- Be tied to approved regional projects that advance KPOs
- Occur in and serve rural areas
Key parameters include:
- Capital costs: Funding used for renovation or alterations cannot exceed 20% of the total funding awarded to the State in each budget period.
| Region | Maximum Capital Expenditures, Budget Period 1 |
|---|---|
| 1 | $4,405,581 |
| 2 | $7,881,614 |
| 3 | $3,960,275 |
| 4 | $6,186,220 |
| 5 | $6,186,220 |
| 6 | $5,238,700 |
| 7 | $4,817,104 |
| 8 | $4,760,479 |
- EMR expenditures: No more than 5% of total funding awarded to the State in a given budget period can support funding the replacement of an EMR system if a previous HITECH certified EMR system is already in place as of Sept. 1, 2025.
| Region | Maximum EMR Replacement Expenditures, Budget Period 1 |
|---|---|
| 1 | $1,101,395 |
| 2 | $1,970,403 |
| 3 | $990,068 |
| 4 | $1,546,555 |
| 5 | $1,033,900 |
| 6 | $1,033,900 |
| 7 | $1,204,276 |
| 8 | $1,190,119 |
- Program costs: Care delivery, workforce, technology, telehealth, transportation solutions, paraprofessional deployment, quality improvement, training, and evaluation are generally allowable when tied to approved projects
- Unallowable costs include: major construction, non-health-related infrastructure, food, general government uses, or activities outside the RHTP scope or service area.
Further details can be found in the RFF.
What is the role of ineligible counties based on HRSA rural health funding? Can those counties still be a subgrantee?
Counties that do not meet the HRSA/FORHP rural definition cannot be the primary target of RHTP investments. However, entities in non-rural counties may participate as subrecipients if their activities clearly:
- Serve rural residents
- Support regional infrastructure or specialty access that rural patients rely on
All funded activities and services must still be rural-serving.
Do regions need to describe how subrecipients will select their contracts and hold those contractors accountable?
Yes. Regional applications must outline:
- Transparent procurement processes for sub-contractors
- How subrecipients will select and monitor vendors
- How performance, data, and compliance will be tracked
- How corrective action will occur if contractors underperform
The state will also impose reporting and audit requirements on subrecipients.
What is considered program duplication? Can funding be used to expand existing programs to include more communities and systems of care?
Program duplication occurs when a new project replicates an existing service or infrastructure without adding value, reach, or efficiency. GROW funds cannot be used to simply replace current funding streams or pay for the same service twice. However, funds can be used to:
- Expand successful programs to additional rural communities
- Add new populations, sites, or modalities (e.g., telehealth, home-based care)
- Integrate programs to reduce fragmentation and improve outcomes
Regions must clearly show how funding fills gaps, scales impact, or increases efficiency, not just continues the status quo.
Does the program limit funding to certain types of providers or facilities?
No single provider type is exclusively favored, but priority is placed on entities that are critical to rural systems, such as:
- CAHs, rural hospitals
- FQHCs and rural health clinics
- CMHCs and CCBHCs
- EMS and mobile integrated health
- Local health departments and CBOs
Proposed funding must support rural-serving entities and align with the required categories and KPOs.
Are regional grants able to fund healthcare services across state borders (e.g., Cincinnati Children’s clinics in Indiana), and how are subrecipient arrangements and lab samples handled when crossing state lines?
Funding may support care models and partnerships that cross state lines if:
- Services are delivered in or clearly serve Indiana rural communities, and
- The arrangement complies with federal and state rules on subawards, licensure and billing.
Cross-border labs, contracts, and subawards must be structured with formal agreements and must still meet all RHTP and Indiana requirements for allowable, rural-serving expenditures.
How should regions consider initiative sustainability after the GROW funding period?
Every regional proposal must include a sustainability plan that addresses:
- How programs will demonstrate ROI or cost savings
- How payers (Medicaid, Medicare, commercial) can support ongoing reimbursement
- How shared services, workforce, and infrastructure will be embedded into routine operations
- How partnerships will persist beyond the grant
Sustainability is a core scoring criterion, not an add-on.
Is the state responsible for issuing RFPs and purchasing resources for regional grants, and if so, how is ownership transitioning to the regions?
All contracts will come directly from the state. The state will:
- Issue state-level procurements for certain supports (e.g., evaluation, technical assistance, some statewide tools).
- Execute grant agreements directly with individual entities carrying out regional activities.
Subrecipients within each region will generally be responsible for their own procurements for needed services within state and federal rules. Ownership of equipment or systems purchased with GROW funds will be defined in the grant agreement but is typically vested in the subrecipient, with conditions for use, reporting, and disposition.
Define subgrantee, subrecipient, subaward, subagreement.
The State of Indiana is the awardee for RHTP funds. The disbursement of these funds to other entities falls into these categories:
- Subrecipient / Subgrantee: An organization that receives GROW funds from the state to carry out a portion of the program (not just to provide goods/services).
- Subaward: The formal award of funds from the state (or primary grantee) to a subrecipient documented in a grant or contract.
- Subagreement: The legal agreement (grant agreement or contract) that outlines the subrecipient’s scope, budget, reporting, and compliance obligations.
Subrecipients may further subaward or procure services via GROW funds, and all additional agreements are subject to state and federal rules.
Can this funding be used for any environmental issues since that impacts health as well?
RHTP funds are not designed to support broad environmental projects, but they can be used for environmental issues when there is a direct and demonstrable connection to rural health outcomes. Environmental activities may be allowable only when they clearly advance a health‑specific objective.
What the funding cannot support are broad environmental initiatives that fall outside the health that don’t have a a clear health impact.
Could neurodegenerative diseases, like Alzheimer's disease, be considered a focused chronic disease?
Yes, they can if the region can demonstrate a clear burden, a rural access gap, and a strategy that aligns with RHTP’s health‑system strengthening goals.
If you were to participate in the regional coalition, would your organization still be eligible to request a sub-award under the regional grant?
Yes.
Could these funds be applied to housing assistance in some capacity to rural areas?
Maybe. RHTP funds cannot be used for broad housing assistance, but they may support housing‑related activities when there is a clear and direct connection to rural health outcomes. Any housing‑focused use of funds must be tightly aligned with the region’s health priorities and must demonstrate a measurable impact on rural health, rather than serving as general housing support.
Will the initial Regional Grant applications cover the entire five-year grant period (similar to the state grant to CMS) or will new applications be submitted each year?
The applications will cover the entire five-year grant period with continuing applications to be submitted each year.
What is considered “Minor alterations or renovations”? Can you explain what sort of additional retrofitting would be permissible under the program versus when it would be impermissible? Is there a “bright line” on when renovations are permissible? Clarify capital expenditures here.
Minor alterations or renovations are small-scale facility changes that support program implementation without constituting major construction or new facility build-out. Examples include:
- Interior reconfiguration of existing clinical space
- Adding exam rooms or telehealth pods
- Upgrading HVAC, electrical, or plumbing to support care delivery
- Accessibility improvements (ramps, doors, restrooms)
The “bright line” is that renovations cannot become large-scale construction, new buildings, or major structural changes. Additionally, total capital costs (including renovations) are limited to 20% of the State’s Budget Period 1 award.
| Region | Maximum Capital Expenditures, Budget Period 1 |
|---|---|
| 1 | $4,405,581 |
| 2 | $7,881,614 |
| 3 | $3,960,275 |
| 4 | $6,186,220 |
| 5 | $6,186,220 |
| 6 | $5,238,700 |
| 7 | $4,817,104 |
| 8 | $4,760,479 |
Further clarification on regional grant renovations and capital expenditures is outlined in the RFF.
Can the program fund renovations or subawards to support housing for training rural students or trainees in healthcare settings?
GROW funds are not intended to function as a housing program. Limited, clearly justified renovations to existing training facilities (e.g., student training spaces in rural clinics or hospitals) may be allowable, but building or renovating housing units purely for lodging trainees would generally fall outside the intended scope. Any proposal in this space would need to:
- Be clearly tied to workforce training capacity
- Fit within capital caps
- Comply with federal construction restrictions
Can GROW money be used to install playgrounds, paths or walking trails in a movement-based initiative to prevent chronic disease like diabetes and obesity?
The program focuses on health care and public health delivery infrastructure, not general recreation infrastructure. While physical activity is a key prevention strategy, GROW funds are unlikely to support stand-alone recreational capital projects (playgrounds, trails) unless:
- They are tightly integrated into a clinical or community care model (e.g., prescribed exercise program)
- They are clearly justified as a minor component of a larger, health-system-led initiative
- They remain within capital caps and federal guidelines
Regions are better positioned to use GROW funds for clinical, telehealth, care coordination, workforce, and evidence-based preventive services, and leverage other funding streams for broader built-environment projects.
To help with the first 11 state initiatives and the cooperation and sharing of patient data, would all hospitals working toward the same modern EMR installation be something that could go possible go over the 5% to help with the expenses of the modernization of the hospitals technology and EMR?
Details about how the regional grants will interact with the 11 state initiatives included in the regional grant applications. The state will consider requests around collaboration and cost allowability on a case-by-case basis.